

This is part of our ongoing series, The Value of Coverage.
Nearly half of all adults in the U.S. have high blood pressure, or hypertension.1 Under current clinical thresholds, three-quarters of these adults do not have their blood pressure under control, which increases the risk for cardiovascular diseases including heart attack, stroke, and heart failure. 2,3
Uncontrolled hypertension is one of the nation’s leading causes of preventable death and disability. It shortens life expectancy, reduces quality of life, and limits workforce participation. In 2019 alone, hypertension accounted for about $219 billion in health care costs, and individuals with hypertension spent an average of $2,800 more than those without the condition.4 Preventing and controlling hypertension through early detection, consistent follow-up, and access to effective could avert thousands of deaths and hospitalizations each year.5
Coverage enables early detection & treatment
Health care coverage – including private insurance, Medicaid, Medicare, and other health insurance – helps people access preventive care, including healthy living resources and screening. This supports early detection, timely medical interventions, and better health outcomes among people with hypertension and cardiovascular diseases.
People without insurance are more likely to be diagnosed later, receive less consistent treatment, not achieve adequate hypertension control, and experiencecomplications like heart attack, stroke, and heart failure.6, 7 According to national data:
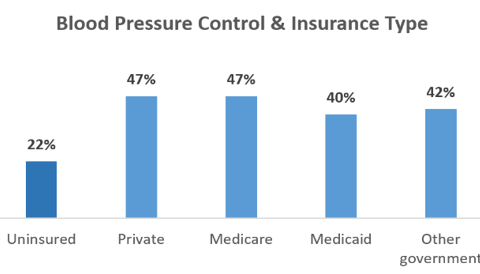
- Hypertension is better controlled among adults with insurance. Hypertension was controlled in just 22% of uninsured adults, compared with 47% among adults with private insurance or Medicare and 40% of adults with Medicaid (see chart).
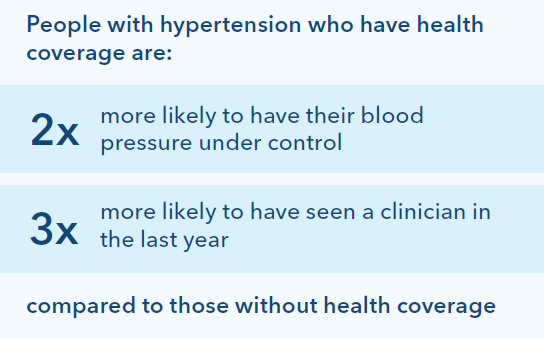
- People with insurance are more likely to see their clinician for hypertension care. Nearly half (46%) of uninsured adults with hypertension had not seen a clinician in the past year, compared with only 15% of insured adults. This limits opportunities for care escalation and disease monitoring.9
- Uninsured adults with hypertension were 61% less likely to take prescribed medication than those with adequate coverage.10 This can worsen outcomes, as antihypertensive medications are most effective when patients can access them consistently.
- Coverage also increases access to cholesterol-lowering medications, which can reduce the risk of heart attack and stroke by roughly 22 and 33%, respectively. Consistent adherence to these medications further improves outcomes and lowers the risk of serious cardiovascular events and mortality. 11
Early, intensive treatment for hypertension can reduce risk of heart attack, stroke, heart failure, and mortality by 25%.12
Coverage is linked to lower risk of heart attack, stroke, and premature death.
Insurance coverage is a critical tool for improving health outcomes. Without the kinds of care that coverage facilitates, hypertension is more likely to be undiagnosed and untreated until serious – sometimes irreversible – damage develops to the heart, kidneys and more. 13,14
Insurance coverage is associated with lower rates of major cardiac events and mortality.15 Uninsured patients are more likely to be hospitalized for heart attack – at a cost of $21,000-$26,000 per hospitalization – and more likely to die after a heart attack. 16, 17
A similar pattern exists for stroke. In one large, multi-year study, uninsured adults had a 65% higher rate of stroke and 26% higher rate of death compared to those with insurance.18
Coverage reduces gaps in care
Hypertension treatment and control remain well below national goals, especially for Black and Hispanic adults, who are less likely to have insurance, be diagnosed and treated appropriately, and have their blood pressure under control.7, 10
Evidence from Medicaid expansion suggests coverage may be a powerful lever for addressing these gaps and improving overall population health. For example, one study of patients who gained insurance coverage found that improvements in blood pressure control rates were 1.5 times greater among Black and Hispanic patients compared to other newly insured patients.19
This is especially important given more Black and Hispanic adults do not have health insurance coverage (11% and 25%, respectively) compared to other groups, such as Asian and White adults (5% and 8%, respectively). 20
The Kaiser Permanente approach
Kaiser Permanente’s value-based integrated care and coverage model supports better cardiovascular health outcomes for our members. 21,22 Our programs emphasize prevention through healthy lifestyle approaches, routine screening for risk factors, and evidence-based treatments. Our care teams, including physicians, nurses, and pharmacists, work together to regularly check blood pressure, make timely medication adjustments, and connect patients with specialized hypertension programs for more hands-on support.
Since unmet social needs – such as food insecurity, unstable housing, and limited transportation – can interfere with medication adherence, follow-up care, and healthy behaviors, care teams are trained to screen patients for social needs and connect them to community resources that help them access safe housing and healthy food.
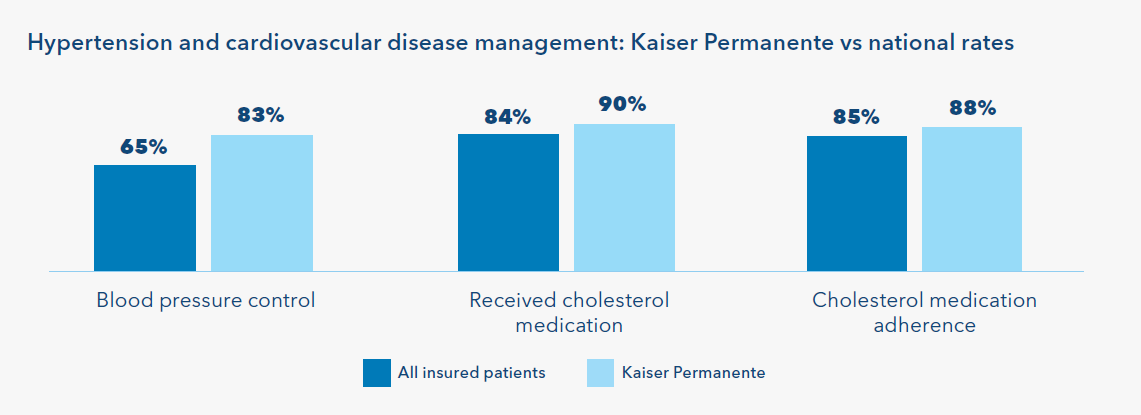
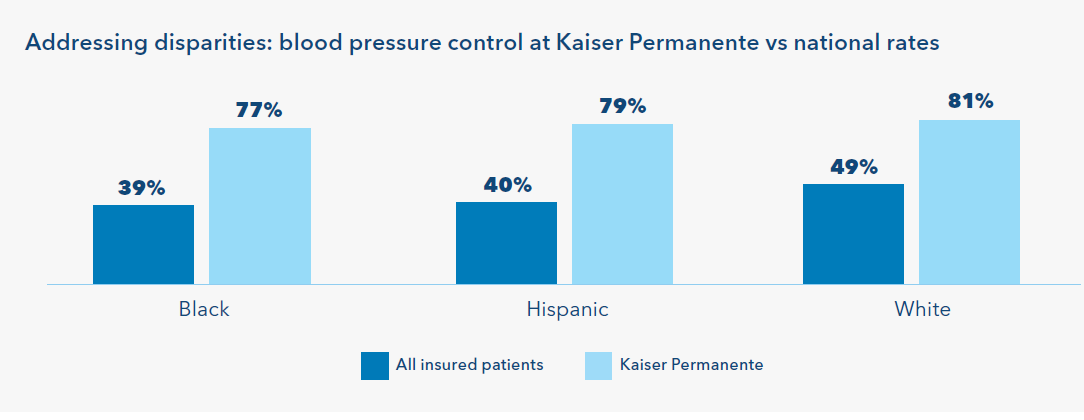
As a result, Kaiser Permanente members experience better care and outcomes compared to all insured patients with hypertension and cardiovascular diseases, our members are more likely to receive and use recommended medications and have controlled blood pressure. (see chart) 23 Kaiser Permanente’s model also supports more equitable outcomes for patients who, on average, experience persistent health disparities. Nationally, Hispanic patients and Black patients with hypertension are approximately 10 percentage points less likely than White patients to have their blood pressure controlled.25 At Kaiser Permanente, Black, Hispanic, and White patients are all more likely to have their blood pressure under control, thanks to quality improvement efforts, innovative care, and strategic research aimed at identifying best practices for addressing preventable differences in outcomes.
Evidence-based care and coverage can save lives. Kaiser Permanente members are 33% less likely to die prematurely from heart disease compared to others living in their communities.24
Health care coverage matters, and integrated care approaches are particularly effective at improving outcomes. Regular screenings and evidence-based treatments support high-quality care, improving health outcomes and reducing both patients’ financial burdens and health care costs to the U.S. health system.