
This is part of our ongoing series, The Value of Coverage.
Cancer is a leading cause of death in the United States and a significant driver of health care costs. In 2025, an estimated 2 million people will be diagnosed with cancer and 618,000 will subsequently have a cancer-related death.1 Cancer incidence is increasing for many common cancers, including 6 of the top 10. Fortunately, some cancers,  including breast, prostate, colorectal, and cervical cancer, can be identified through screening.2 Health coverage is critical to ensuring these screenings occur.
including breast, prostate, colorectal, and cervical cancer, can be identified through screening.2 Health coverage is critical to ensuring these screenings occur.
Cancer care is most effective with early prevention and treatment
Prevention and treatment advances can extend lives. Smoking-cessation programs, earlier cancer detection, and improved treatments have helped reduce the cancer death rates by 33% over the past 3 decades.3 Late-stage cancer diagnoses remain common, however, leading to more invasive treatments, higher costs, worse health outcomes, and greater financial strain for both consumers and the overall health system.4 For example, in the first year of breast cancer treatment, the average cost of treating more localized breast cancer is $60,637 for stage 0 cancer or $82,121 for stage 1 or 2, while treatment costs are higher for later stage breast cancer ($129,387 for stage 3 and $134,682 for stage 4).5 Experts estimate that earlier cancer detection could save the U.S. health care system an estimated $26 billion annually.6
 Health care coverage is essential for cancer detection and care
Health care coverage is essential for cancer detection and care
Health care coverage —including private insurance, Medicare, Medicaid and other public insurance — helps people to access preventive care supports and early treatment, supporting early detection and timely medical interventions. Individuals with health insurance are far more likely to receive regular medical care, including preventive screenings. For example, people without insurance are less likely than people with insurance to get screened for breast cancer, cervical cancer, or colorectal cancer (see charts).7 These screenings help avoid delayed diagnosis and the progression toward more advanced-stage disease that can reduce treatment success.
The Kaiser Permanente approach
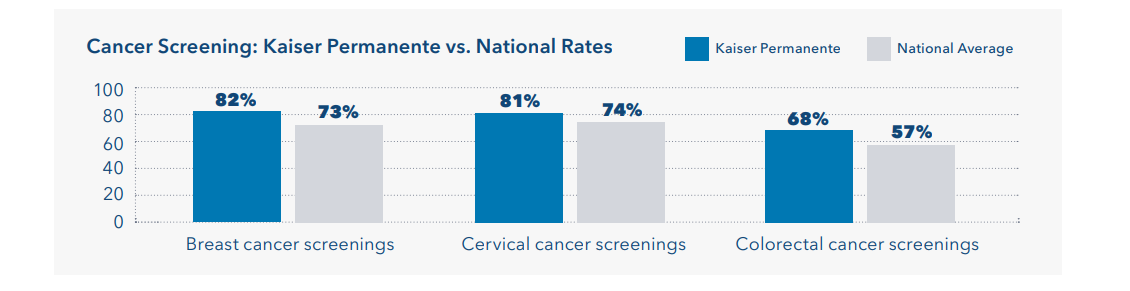
Kaiser Permanente screening rates are even higher than average, compared to national screening rates for breast cancer (82% vs. 73%), cervical cancer (81% vs. 74%), and colorectal cancer (68% vs. 57%).8
 With our integrated care approach, we ensure members are actively encouraged and reminded to have cancer screenings. We integrate screenings into routine care visits, ensuring that patients have multiple opportunities to undergo necessary tests. For example, automated mammogram scheduling supports breast cancer detection, while mail-in test kits improve colorectal cancer screening convenience.
With our integrated care approach, we ensure members are actively encouraged and reminded to have cancer screenings. We integrate screenings into routine care visits, ensuring that patients have multiple opportunities to undergo necessary tests. For example, automated mammogram scheduling supports breast cancer detection, while mail-in test kits improve colorectal cancer screening convenience.
We use electronic health records to track patient history, flag overdue screenings, and send automatic reminders to both members and physicians. Outreach teams engage at-risk populations, addressing barriers such as language, transportation, and health literacy. We also recognize the importance of patient engagement – explaining the screening process, emphasizing its benefits, and sharing information about follow-up care provided for any positive screenings. These steps help us detect cancer earlier, improving treatment success rates and overall health outcomes.
Early detection, enabled by coverage, saves lives
When cancer is identified through screening, we ensure timely and effective cancer treatment through multidisciplinary teams, including oncologists, radiologists, and care coordinators. These care teams develop personalized treatment plans using the latest evidence and advances. We provide coordinated care that includes cutting-edge treatments, access to clinical trials, and supportive services such as nutrition counseling and mental health support.
Health care coverage matters, and integrated care approaches are particularly effective at improving outcomes. Higher screening rates lead to earlierinterventions, improving health outcomes and reducing both patients’ financial burdens and health care costs to the U.S. health system.